 This site will focus on potential mechanisms of hyperacusis caused by sound exposure. Much of what is discussed is still relevant to other causes of hyperacusis. The material is split into four sections:
This site will focus on potential mechanisms of hyperacusis caused by sound exposure. Much of what is discussed is still relevant to other causes of hyperacusis. The material is split into four sections:
Before starting, you may want to review how the ear works.
Potential Mechanisms Overview
None of the potential mechanisms have been proven but each year researchers add to the growing body of knowledge on the subject.
- Symptoms such as aural fullness (ear pressure), muffled hearing, tympanic flutter, and some types of ear pain are common for those who develop hyperacusis. This collection of symptoms is called Tonic Tensor Tympani Syndrome (TTTS) and can be caused by the unusual activation of middle ear muscles that function to dampen sound and protect hearing. The hyperactive and prolonged contraction of these muscles is likely triggered by an unusual increase in activity in the central auditory system. These TTTS contractions are likely worsened by the urge to protect one’s own ears from sound.
- Central Auditory System hyperactivity is thought to contribute to tinnitus, loudness hyperacusis and possibly pain symptoms.
- Damage to the Inner Ear might be why the hyperactivity starts in the first place. Cochlear damage has been shown to trigger abnormal, hyperacusis-like hyperactivity in the central auditory system in animals. This is often coarsely described as an increase in auditory gain.
- Recent studies have found nerves in the cochlea that are behaving like pain receptors. These nerves or their neurological processing centers may play a role in hyperacusis pain symptoms.
- Discovery of potential pain receptors in the cochlea has created some suspicion that pain hyperacusis may primarily be a peripheral phenomenon. The sensations that come with pain hyperacusis make a peripheral explanation more intuitive:
- Pain is localized to the ears
- Pain can be much worse in one ear
- Just as too much weight on a bad ankle can cause re-injury, sound exposure can cause setbacks that feel damaging. Lingering pain and reduced pain thresholds can take days, weeks, or longer to recover.
- However, many researchers suspect this could instead be referred pain or pain triggered as a result of disfunction in the central auditory system. There are several reasons for this:
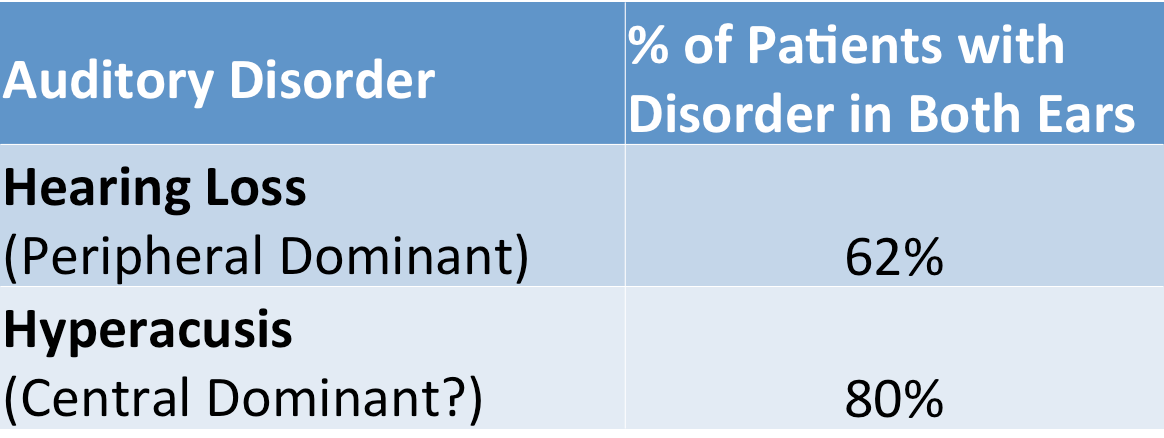
- Although hyperacusis symptoms can be worse in one ear, it occurs in both ears more often than peripheral disorders such as hearing loss.

Hyperacusis data from (Anari 1999, Juris 2013, Westcott 2013).Click to Show: Discussion
Studies so far have not split pain and loudness hyperacusis results. Although some studies show a high percentage of pain symptoms in hyperacusis patients (88% Anari) others show a lower percentage (45% Juris). As a result, there is a possibility that there are fewer cases of pain hyperacusis in both ears than suggested by the overall data.
Reports of unilateral hyperacusis have been very inconsistent. Some authors who publish studies on TRT (Formby, Jastreboff) mention that there are no such cases or that it is very rare. However others (Anari, Westcott) noted that up to 27% of patients reported symptoms in only one ear. The difference between the two may arise as a result of Formby and Jastreboff studies using LDLs to determine bilateral hyperacusis while Anari and Westcott noted patient reported symptoms. It is possible that LDLs in a “good” ear are set based on levels intended to protect the “bad” ear. It is also possible that those with hyperacusis much worse in one ear did not report the symptoms that can arise less often in the “good” ear. Either way, this is an important discrepancy that needs an explanation.
- The cochlea is frequency selective. When noise damages the cochlea and causes hearing loss, this impacts specific frequency regions that can be identified in a hearing sensitivity test. If cochlear damage directly translated to pain and discomfort, measured loudness discomfort levels would be expected to reside in specific frequency regions. Instead, loudness discomfort levels of hyperacusis patients are generally lowered across frequency regardless of hearing loss (at least up to 8kHz) (Sheldrake 2015). This hints at a neurological explanation or a systemic lowering of pain thresholds.
Click to Show: Discussion
Tinnitus and hyperacusis researchers generally only test up to 8kHz which is about half of the full audible frequency range (up to 20kHz). While the Sheldrake study shows similar discomfort levels across frequency up to 6 kHz, there is a 7 dB drop in average LDL from 6 kHz to 8 kHz. Do LDLs continue to drop as frequency is increased to higher audible frequencies? If so, this would show frequency selectivity and match the subjective reports of high frequency sensitivity among hyperacusis patients. A comparison with a control group at these frequencies would be necessary.
Hyperacusis patients are often provided broadband noise for therapy. Noise types that have more high frequency content are known to cause greater irritation. At similar loudness levels, white noise is more irritating than pink noise. Pink noise is more irritating than brown noise. This is inconsistent with the assumption that discomfort is frequency independent.
There are a few other possibilities that might explain how cochlear damage might result in little LDL variation across frequency. First, higher intensity sounds excite broader regions of the cochlea than low intensity sounds. Second, LDLs do not measure pain thresholds. There is a possibility that pain thresholds can become more strongly frequency dependent after damage while the conscious judgment of when sound is too loud does not depend strongly on frequency. Third, systemic damage to the cochlea, possibly through changes in fluid regulation or development of conductive hyperacusis, might result in uniform changes throughout the cochlea.
Whether or not cochlear damage triggers discomfort directly is still being investigated. What is certain is that cochlear damage can trigger hyperactivity in the central auditory system.
- Although symptoms are not always symmetrical, hyperacusis often occurs suddenly and bilaterally (in both ears). If peripheral disfunction was the sole mechanism of hyperacusis, it would be expected that each ear would drop suddenly in loudness tolerance at different times. Hyperacusis occurs suddenly (and usually bilaterally) in 50%-60% of cases (Anari 1999, Juris 2013).
- Although hyperacusis symptoms can be worse in one ear, it occurs in both ears more often than peripheral disorders such as hearing loss.
More can be learned about these potential mechanisms by stepping through the links below:



Have ideas on how to make this article better? Please contact improve@hyperacusisfocus.org.
References
Anari M, Axelsson Alf, Eliasson A, Magnusson L. Hypersensitivity to Sound: Questionnaire data, audiometry and classification. Scand Audiol 1999:28:219-230.
Auerbach B, Rodrigues P, Salvi R. Central gain control in tinnitus and hyperacusis. Frontiers in Neurology 2014:5:206(1-21).
Flores E, Duggan A, Madathany T, Hogan A, Marquez F, Kumar G, Seal R, Edwards R, Liberman MC, Garcia-Anoveros J. A Non-cononical Pathway from Cochlea to Brain Signals Tissue-Damaging Noise. Current Biology 2015:25:1-7.
Juris L. Hyperacusis: Clinical Studies and Effect of Cognitive Behavioral Therapy. Uppsala Dissertations from the Faculty of Medicine 2013:934:1-64.
Lin F, Niparko J, Ferrucci L. Hearing Loss Prevalence in the United States. Arch Intern Med 2011:171(20):1851-1852.
Pienkowski M, Tyler R et. al. A Review of Hyperacusis and Future Directions: Part II. Measurement, Mechanisms, and Treatment. American Journal of Audiology 2014:23:420-436.
Sheldrake J, Diehl P, Schaette R. Audiometric characteristics of hyperacusis patients. Frontiers in Neurology 2015:6(105):1-7.
Westcott M et. al. Tonic tensor tympani syndrome in tinnitus and hyperacusis patients: A multi-clinic prevalence study. Noise & Health 2013:15:117-128.